


INTRODUCTION
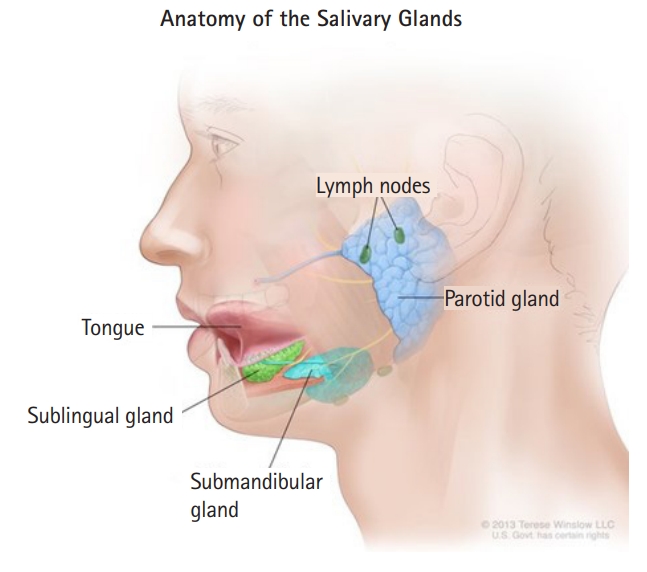
The submandibular gland (SMG) is a salivary gland that is located within the submandibular triangle, also known as the digastric triangle (Fig. 1) [1]. The SMG is innervated by the chorda tympani branch of the facial nerve (seventh cranial nerve). Blood is supplied to the SMG by branches of the facial artery, and blood is returned to the bloodstream by corresponding branches of the facial vein along with the sublingual vein. Traumatic injury involving the SMG is rare due to its protected anatomical position behind the mandible. To the best of our knowledge, only two other case reports have been published with a similar injury; specifically, the American Journal of Otolaryngology reported an SMG injury as a result of seat belt trauma in 2009 [2], and the British Journal of Plastic Surgery also reported a case of SMG trauma because of high-voltage burns [3]. Outside of these cases, the literature is theoretical only. Due to the scarcity of these injuries, we feel that the following case study is a valuable record. Additionally, the study of this injury raises questions about appropriate airway and hemodynamic management. Written informed consent was obtained.
CASE REPORT
A 67-year-old female with no significant past medical history suffered a ground-level mechanical fall that caused her to land on a watering can, resulting in a small puncture wound to the left anterolateral base of the neck, angled superiorly from the base of her mandible. Paramedics on the scene reported that the patient was found on the floor in a large pool of blood. Their primary assessment showed that the patient was pale, cool to the touch, and had thready distal pulses. The first set of vital signs was concerning for hemorrhagic shock. The patient's blood pressure was 60/23 mmHg, with a pulse of 133 and an oxygen saturation of 97% on room air. The paramedics started large-bore intravenous lines bilaterally and gave the patient 1 L of 0.9% sodium chloride and 1 g of tranexamic acid (TXA), which seemed to control the external bleeding. However, they noticed that she continued to have intraoral bleeding. Due to copious amounts of blood coming from the airway, she was intubated for airway protection. The patient was then flown to a local trauma center. She was given two units of packed red blood cells and fresh frozen plasma. A head and neck computed tomography scan was concerning for a possible SMG injury. The trauma surgeon was able to directly visualize a left SMG injury in addition to an external jugular vein laceration. The patient was admitted to the intensive care unit, where the surgeon repaired the laceration. She remained intubated due to concerns about airway swelling and extrinsic compression. After the second day of intensive care unit admission, the patient was safely extubated and was then discharged home the following day with a prescription for prophylactic antibiotics and steroids. At the time of this review, the patient suffered from a loss of taste and a subtle left marginal mandibular branch facial nerve palsy, causing slight lower lip asymmetry.
DISCUSSION
This case illustrates an injury that is not often encountered and is documented only in very few reports. The location of the injury brings unique concerns for hemorrhage and airway management. Most existing literature recommends surgical management of the bleeding, but this recommendation is based heavily on theoretical considerations. The medical management of bleeding in this patient with external pressure and TXA brings an added component to treating SMG-related hemorrhage. Transporting the patient to the nearest appropriate trauma center is still exemplary care, but medication administration, when appropriate, should not be overlooked as it played a large part in this patient's outcome. SMG trauma may require immediate airway protection due to significant bleeding, hemoptysis, and distorted neck anatomy [4]. Additionally, as seen with this patient, SMG trauma can result in delayed airway compromise. If intubation is withheld, providers should be aware that the progression of airway swelling has been documented in cases up to 36 hours after the event [5]. If intubation is withheld, it should be noted that an expanding hematoma across the cricoid membrane could quickly develop, which is a relative contraindication to cricothyrotomy and potentially detrimental to the patient [6]. This case is unique in the fact that SMG trauma is a rare occurrence, but it also shows the importance of prompt airway management in cases of neck trauma.