Cost-effective cardiopulmonary resuscitation practice device for maintaining chest compression quality: a semi-randomized controlled clinical trial
Article information

Abstract
Objective
Continued chest compression after the completion of a basic life support (BLS) course is effective for maintaining the skills acquired during the course. Using low-cost tennis balls for BLS practice, we examined the effects on the long-term continued quality of chest compression.
Methods
This semi-randomized controlled clinical trial included 153 participants who completed BLS courses from August 2018 to December 2019 and were randomly divided into 5 groups: ball with rhythm (n=33), ball without rhythm (n=32), manikin (Little Anne) with rhythm (n=16), manikin without rhythm (n=23), and no-practice (n=49). Immediately after training and at 3, 6, and 12 months following training, chest compression quality (rate, depth, recoil, and pressure point) was measured, and intergroup comparisons were statistically analyzed.
Results
The no-practice group demonstrated a decline in chest compression quality at 3 months after BLS course completion. However, no participant in the ball with rhythm group demonstrated a decline in quality on any evaluated items even at 12 months. The tennis ball group (n=65) and the manikin group (n=39) did not demonstrate any significant differences in chest compression quality.
Conclusion
Weekly BLS practice with low-cost tennis balls can maintain the quality of chest compression for 12 months. Tennis balls are spherical, give only on perpendicular downward compression, and roll away on removing hands, which facilitates the acquisition of proper chest compression posture. Weekly practice is important for skill maintenance following the completion of the BLS course.
INTRODUCTION
Rapid, effective chest compressions are needed to increase the rate of return of spontaneous circulation in patients with cardiac arrest [1]. In its 2020 guideline, the Japan Resuscitation Council similarly clarified the crucial importance of high-quality chest compression [2]. The Japan Advanced Cardiovascular Life Support Association has established a 2-year licensing option for students of classes on chest compression and other forms of basic life support (BLS) education as well as a renewal of this BLS license every 2 years [3]. However, the knowledge and skills obtained in BLS courses rapidly decline after the completion of the course, raising doubts as to whether 2 years is a suitable interval for license renewal. These doubts are bolstered by the findings of a study conducted by Oermann et al. [4], who stated that, without subsequent chest compression practice, the quality of chest compression depth declines greatly within 9 to 12 months after the completion of a BLS course. Furthermore, Anderson et al. [5] similarly reported that the quality of chest compression declines without practice for 3 to 6 months. These studies have shown that 2 years is an utterly unsuitable interval for license renewal, and that repeated practice after the conclusion of BLS courses is necessary for preventing a decline in the chest compression quality.
The 2020 Japan Resuscitation Council guideline, which is the most recent version, emphasizes the need for re-training within 1 year, rather than after every 2 years [2]. However, the coronavirus disease 2019 (COVID-19) pandemic has hindered conventional instructor-led, face-to-face cardiopulmonary resuscitation (CPR) training worldwide. In fact, BLS courses have often been cancelled, and even conventional renewal courses that were earlier held at 2-year intervals have become seemingly impossible. Factors, such as the decline in trainees’ skills over time and difficulties in completing courses due to the COVID-19 pandemic, highlight the need for a framework wherein individuals can cost-effectively self-learn BLS skills through repetitive practice rather than from an instructor.
In the present study, we aimed to demonstrate that chest compression can be practiced effectively with common items to develop a means for encouraging repeated chest compression practice following BLS course completion and to evaluate the effects of this repeated practice in CPR training.
METHODS
Study design and participants
This study is a prospective, semi-randomized comparative study that enrolled 236 participants who had completed a BLS course. The BLS course was conducted from August 2018 to December 2019. The participants were recruited from Matsunami General Hospital and Tokai Gakuin University. The participants from A Hospital included 61 out of 80 employees, after excluding physicians and nurses who would routinely perform CPR in the course of their duties. The participants from Tokai Gakuin University comprised 175 out of 200 students, after excluding students who planned to become emergency medical technicians as they were undergoing chest compression training outside of the practice for the study. Thus, in total, 236 potential participants were screened from the 2 study centers and they underwent the BLS course. Data from 153 participants were analyzed.
Data collection
Participants received training in a 2-hour course covering chest compression, ventilation, and the use of an automated external defibrillator. At course completion, we measured the quality of the chest compressions delivered by the participants with regard to depth, rate, recoil, and pressure point, as well as an overall score, which was the sum of the mean scores of the above-mentioned items. The measurements were obtained through the Shinnosuke-kun chest compression training evaluation system [6] (model number SVWB1321J; Sumitomo Riko Co., Ltd., Nagoya, Japan).
For all BLS courses, the content, duration, and instructors were identical. Following the conclusion of the courses, participants were randomly divided into 5 groups: 4 groups engaged in repeated practice. Participants who engaged in a 5-minute chest compression practice session every week with a tennis ball were defined as the tennis ball group, which was further divided into 2 subgroups: participants who practiced while listening to a rhythm of 110 beats per minute (ball with rhythm group, n=46) and participants who did not listen to this rhythm (ball without rhythm group, n=47). Only hard tennis balls (Bridgestone Non-Pressure Balls; ISBN code: 4547333764040; Bridgestone Corporation, Tokyo, Japan) were used for the practice. Participants were instructed to put pressure on the balls until they dent the ball to the end. In the manikin group, repeated practice involved a 5-minute chest compression practice session once per week with a chest compression practice manikin (Little Anne QCPR, part number: W19646; Laderal Medical, Stavanger, Norway). The manikin group was further divided into 2 subgroups: participants who practiced while listening to a rhythm of 110 beats per minute (manikin with rhythm group, n=30) and participants who did not listen to this rhythm (manikin without rhythm group, n=30). The fifth group was the no-practice group (n=82), in which participants did not engage in any chest compression practice whatsoever. Tennis balls were chosen as chest compression practice devices for the following reasons: their spherical shape means that they can only be pushed from directly above, trainees can learn the proper direction to compress the sternum, the balls take up almost no space during practice, and they are inexpensive, lightweight, and easily portable.
Based on the response to our enquiry made to Bridgestone about the performance of the Bridgestone Non-Pressure Tennis Balls used in the study, we learned that producing 1 cm of give required roughly 15 kg force, the maximum give was 3.3 cm, and obtaining this maximum give required 49.5 kg of force. This pressure for producing give in the tennis ball is nearly identical to the finding by Tomlinson et al.[7] that reaching a compression depth of 5 cm in chest compression required 50 kg force. These reasons support our selection of Bridgestone Non-Pressure Tennis Balls for CPR practice in the present study.
Using the Little Anne manikin and the Shinnosuke-kun, we measured chest compression again for 1 minute immediately after and at 3, 6, and 12 months following the conclusion of the BLS course. Based on these measurements, we compared the intragroup changes in chest compression quality from the baseline to the assessment timepoints. We sought to examine whether a tennis ball could serve as a chest compression practice device by proving that practicing chest compression with a tennis ball would prevent decline in the quality of chest compression and that the ball was comparable to the Little Anne manikin in terms of practice effect.
The Shinnosuke-kun measures chest compression quality by determining whether the numerical values for each push meet the guideline target values for all items, with the score for each item represented as a percentage of how frequently the target value was reached (with 100 points being a perfect score). We chose to use the Shinnosuke-kun to measure chest compression based on a study by Minami et al. [8].
Statistical analysis and ethical considerations
Statistical analysis was conducted with Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). Measurements obtained immediately after the conclusion of BLS courses (hereafter, “baseline”) and subsequent measurements in each group were compared using a paired t-test. Comparisons (conducted with JMP PRO 15; SAS Institute Inc., Cary, NC, USA) at 12 months after BLS course conclusion were performed with one-way analysis of variance owing to differences in the numbers of participants, whereas multiple comparisons were performed with Dunnett’s test. Values of P<0.05 were considered significant.
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Kokushikan University (approval no: 18005 and date of 14 June 2018), and all participants provided written informed consent for participation. Participation in the study was strictly voluntary, and those who did not wish to continue the study after it had started were treated as dropouts. The data used in the present study did not include any data that could be used to identify individual participants, and their privacy was protected.
RESULTS
Participants
Of the 236 participants, 83 (28 in the tennis ball group, 22 in the manikin group, and 33 in the no-practice group) stopped participating in the practice and measurement sessions during the study and were treated as dropouts. Thus, we were able to obtain data for a 12-month period following the conclusion of BLS courses from 153 participants. This cohort comprised 33, 32, 16, 23, and 49 participants in the ball with rhythm, ball without rhythm, manikin with rhythm, manikin without rhythm, and no-practice groups, respectively (Fig. 1).

Categorization of the study subgroups and the number of participants in each group.
Chest compression in the tennis ball group (ball with rhythm and ball without rhythm subgroups) at 3, 6, and 12 months
Comparisons in the ball with rhythm group between baseline and 12 months revealed no significant differences in any of the measured items. However, comparisons between the measurements at the baseline and at 12 months in the ball without rhythm subgroup revealed a significant decrease in the chest compression rate (P=0.004) (Table 1).

Intragroup comparison of the parameters at the baseline and at 12 months in the tennis ball group
In the tennis ball group, the chest compression style of most participants at 12 months involved the application of force perpendicular to the sternum; however, the Shinnosuke-kun force sensor, which shows the spread of force, did not show a spread of force larger than the base of the palm in any participant (Fig. 2). In addition, most participants correctly pushed the sternum with the base of the palm and relieved pressure during the examinations of compression technique without removing their hands from the sternum.
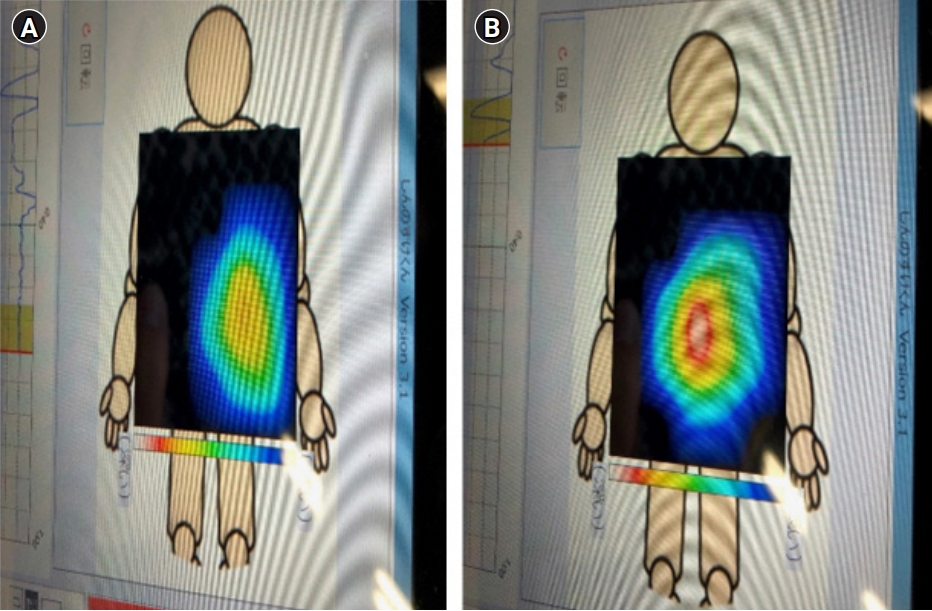
Shinnosuke-kun pressure-sensor readings during chest compression in the no-practice group (A) and the tennis ball group (B). The red area indicates the correct compression pressure (5–6 cm). The right side indicates the tennis ball group, with the correct compression pressure in the center of the sternum.
Chest compression results in the manikin group (manikin with rhythm and manikin without rhythm subgroups) at 3, 6, and 12 months
Comparisons in the manikin with rhythm group from the baseline to measurements at 12 months revealed no significant differences in any measured items. However, comparisons between baseline and 12 months in the manikin without rhythm group revealed a significant decrease in the chest compression rate (P<0.001) (Table 2).
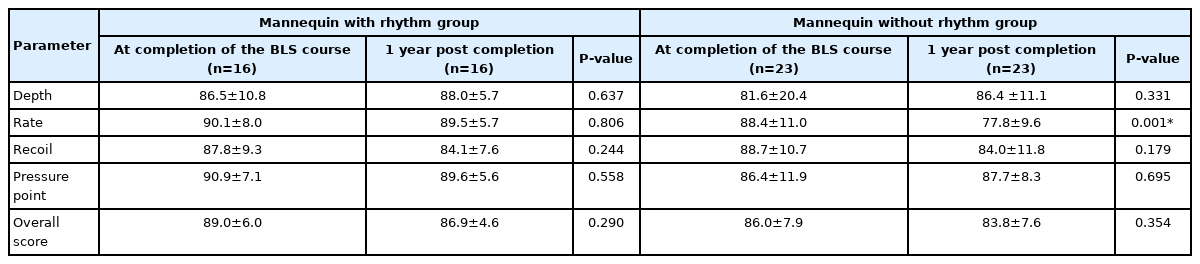
Intragroup comparison of the parameters at the baseline and at 12 months in the manikin group
Chest compression results in the no-practice group at 3, 6, and 12 months
At 3 months, the no-practice group demonstrated a significant decline in all parameters other than depth. However, even the compression depth declined significantly at 6 months compared with the baseline (Table 3).

Intragroup comparison of the parameters at the baseline to those at 3 and 6 months in the no-practice group
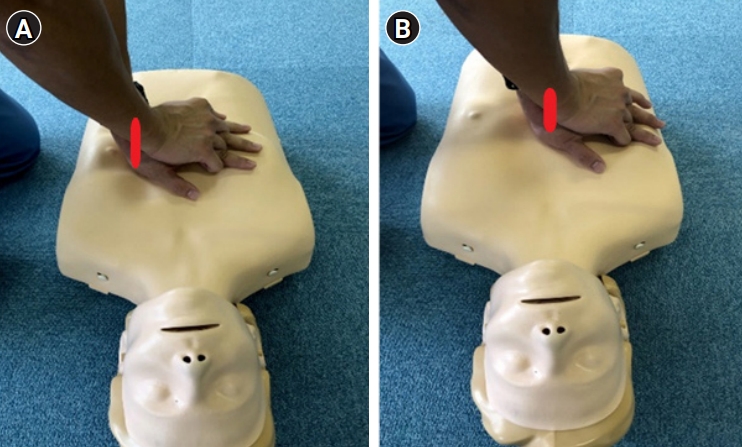
Chest compression style for most participants in the no-practice group at 12 months involved pushing diagonally (Fig. 3), with the force sensor showing horizontal extension of force. Pressure was applied not with the base of the palm but rather with the center of the palm. In addition, most participants removed their hands from the sternum following each push during examinations of the compression technique (Fig. 4).

Direction of compression in chest compression in the no-practice group (A) and the tennis ball group (B).
Position of the hands during chest compression in the no-practice group (A) and the tennis ball group (B).
Comparisons between the tennis ball and the manikin groups
Practice effects in the tennis ball and the manikin group were compared with regard to the overall score at 12 months. Analysis of variance in the ball with rhythm, ball without rhythm, manikin with rhythm, and manikin without rhythm groups revealed significant differences in the chest compression depth, rate, pressure point, and overall score; recoil was the only item for which a significant difference was not observed (Table 4).
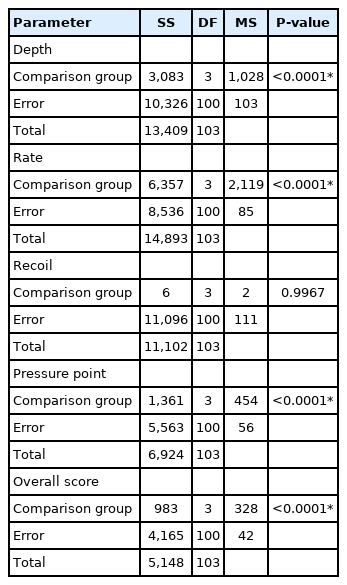
Results of the one-way analysis of variance for the 4 repeated practice groups
In multiple comparisons of the ball with rhythm group (as a control) with the other 3 repeated practice groups, the chest compression depth, rate, and overall score increased significantly in the ball without rhythm group. However, in the manikin with rhythm group, a significant difference was observed only in the pressure point (Table 5).
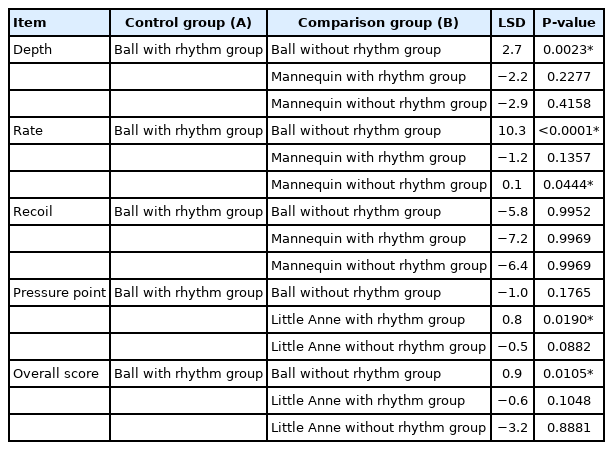
Dunnett’s test using the ball with rhythm group as the control group
DISCUSSION
In the present study, we found that practicing chest compressions by using a tennis ball effectively ensured sustained CPR quality in the long term. The no-practice group demonstrated significant differences in all items other than the chest compression depth at 3 months and did not maintain chest compression quality over the course of 12 months. However, in the tennis ball and manikin groups (i.e., the repeated practice groups), practicing while listening to a rhythm allowed participants to maintain chest compression quality for all parameters over the 12-month study period.
Conceivably, the reason that practice with a tennis ball enabled participants to maintain chest compression quality is that they learned to apply the proper amount of force because the force required to yield maximum give in the tennis balls used in the study is identical to the force required to depress the sternum to the 5-cm depth required in chest compressions. In addition, tennis balls are designed to be tougher than human skin and muscle, not to give when pushed with the center of the palm, and to give under force that is applied with the base of the palm. Therefore, practicing with tennis balls is surmised to have taught participants to compress the chest with the base of the palm, which is a more natural and proper contact area for chest compression. Furthermore, we learned that, in practicing with a tennis ball, practicing while listening to a guideline-recommended proper rhythm enabled participants to apply force more deeply and correctly. Zimmerman et al.[9] reported similar findings that the rate of chest compressions can be optimized by using a metronome. Thus, we demonstrated that listening to a proper rhythm while practicing chest compression helped trainees to learn the correct rate and depth of chest compression.
In the tennis ball group, the rationale for the participants being able to relieve pressure during recoil action for examination of compression technique without removing their hands from the sternum is that tennis balls are spherical, which means that removing the hands from the ball upon each recoil during compression will cause the ball to move, thereby hindering the application of force. This factor may have contributed to why participants in the tennis ball group did not change the position of their hands at any point. However, in the no-practice group, we demonstrated that, with participants who removed their hands from the sternum, the position of their hands gradually deviated from the initial position, meaning that the pressure point was liable to change, and this factor may have led to the incorrect pressure point. Furthermore, in the tennis ball group, most of the participants correctly applied compression from directly above the sternum. As tennis balls are spherical, they will roll away if compressed diagonally, which is conceivably why participants in the tennis ball group learned to compress the balls from directly above. In addition, as reported by Hightower et al. [10], performing chest compression with correct posture is surmised to involve less fatigue than with compression that is applied diagonally.
Comparisons between the effects of practice with a tennis ball and a manikin in the present study revealed that the ball with rhythm group and the manikin with rhythm group did not differ significantly with regard to the overall score, which is the mean of all other parameters. This implies that the effect of practicing chest compression with a tennis ball does not differ overall from the effect of practicing CPR with a manikin. This result signifies that practice with an expensive Little Anne manikin can be substituted with practice with a tennis ball, which can be performed easily and inexpensively while alone at home and without taking up space. The Little Anne manikin can be compressed for 5−6 cm and can also be used to practice ventilation, which easily makes it the superior practice device. However, a Little Anne manikin costs $300, making it difficult to purchase and use for individual practice at home or elsewhere. In contrast, a tennis ball costs only approximately $1 and yields a practice effect that is identical to that of a Little Anne manikin, which are factors that conceivably make tennis balls a cost-effective CPR practice tool. Last year, a presentation concerning the efficacy of chest compression practice with tennis balls was shared at the annual meeting of the Japanese Association for Acute Medicine, and members of the Organizing Committee for the Olympics/Paralympics who attended the presentation subsequently incorporated our tennis ball-based chest compression practice in CPR classes for volunteers in the Tokyo Olympics. The proposed method has also been used in CPR e-learning programs.
Furthermore, we examined the long-term durability of tennis balls as devices for individual chest compression practice. Although the felt on the outside of the ball had slightly worn off, the non-pressure nature of the balls meant that the internal air pressure remained constant, and the balls could still be used for practice at 12 months with the same elasticity. However, we have not examined balls from manufacturers other than the Bridgestone balls that were used by the tennis ball group in the present study; thus, the durability of tennis balls from other manufacturers for practice over 12 months remains unknown. The durability of the tennis balls used in CPR practice over a 2-year period, which is the current interval until re-training, must be examined in future studies.
In summary, the present study showed that chest compression quality declines within 3 months after the conclusion of a BLS course without repeated chest compression practice, whereas practicing with a tennis ball for approximately 5 minutes once per week can prevent a decline in chest compression quality over the course of 12 months.
Although it is important to shorten the period until BLS license renewal, we would like to emphasize that, with courses themselves being currently delayed due to COVID-19, repeated practice of the chest compression technique learned in BLS courses potentially prevents a decline in chest compression quality after the conclusion of the course and may improve survival rates for patients who suffer cardiac arrest.
With the use of a tennis ball, which is easily portable, chest compression can be practiced anywhere on a hard surface. Furthermore, we learned that practice with a tennis ball yields nearly the same effect as practice with a Little Anne manikin. In 2022, with COVID-19 wreaking havoc worldwide, holding conventional BLS courses is no longer feasible.
We propose chest compression training that involves not only remote BLS courses but also tennis ball-based practice, which can be performed easily, economically, and individually. This procedure can maintain chest compression quality as a mode of training that meets the needs of the times, both now and in the future.
Notes
Funding
None.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Authors’ contributions
Conceptualization: YA; Formal analysis: YA, Hiroshi Takyu; Investigation: YA; Methodology: YA, Hiroshi Takyu, Hideharu Tanaka; Project administration: YA, Hiroshi Takyu, Hideharu Tanaka; Supervision: Hideharu Tanaka; Validation: YA; Visualization: YA; Writing–original draft: YA; Writing–review & editing: YA.