


INTRODUCTION
Neurological damage after resuscitation in out-of-hospital cardiac arrest (OHCA) patients induced poor outcomes or death [1]. Much effort has been made to reduce neurological damage in OHCA patients, of which targeted temperature management (TTM) has been shown to be excellent in reducing neurological damage in post-resuscitation treatment [2,3]. Although the exact mechanism of TTM is still unclear, previous studies have speculated that it works through the modes of inhibiting ischemia-reperfusion injury, mitigating intracranial hypertension, reducing brain edema, and stimulating the protective system [4,5].
A human body temperature (BT) is regulated by the hypothalamus between 35.5°C and 37.5°C, and this regulation is essential for sustain life [6,7]. If BT is not properly controlled, it can cause fatal damage to the patient. Major trauma, such as increased mortality in patients with low BT, is associated with impaired body temperature control and unfavorable neurologic recovery [8−10]. Association of low BT with unfavorable outcomes has also been reported in other neurologic problems [11,12].
Initial BT of OHCA patients could be affected by various conditions. It could be associated with the circumstance of arrest, especially for the place of arrest. It could also reflect neurologic damage that could result from impairment of BT regulation [13]. A previous study showed that low initial BT was associated with mortality in OHCA patients who underwent TTM [14]. However, it was a single-center study, with a relatively small sample size, and therefore lacks generalisability. In addition, because a previous study mainly focused on the comparison of BT between survivors and non-survivors, the effect of low or high initial BT compared to normal initial BT for survival outcomes is unclear.
The aim of this study was to investigate the association between initial BT and neurological outcomes in OHCA patients who underwent TTM. We hypothesized that survival outcomes of patients with low or high initial BT compared to normal initial BT would be poor. We also examined whether the association differed based on initial ECG.
METHODS
Study design, data source and setting
This study was a cross-sectional observational study using nationwide OHCA registry. Nationwide OHCA registry of Korea was initiated in collaboration with National Fire Agency and Korea Centers for Disease Control and Prevention (KCDC). This registry collects information of all emergency medical services (EMS)-assessed OHCA occurred from Korea, drawn from the following four sources: the EMS run sheets, the EMS cardiopulmonary resuscitation (CPR) registry, the dispatcher CPR registry, and the medical record review by KCDC for hospital care and outcomes. The quality management committees (emergency physicians, epidemiologists, statistical experts, and medical record review experts) analyse the data collected every month and feedback to improve the quality of medical records. Detailed information for registry and quality control process was previously published [15,16].
The National Fire Agency of Korea controls EMS, provides basic-to-intermediate ambulance services [17,18]. The national government has designated three kinds of emergency departments (ED): regional emergency medical center (EMC) (n=36), emergency care is provided by emergency specialists 24 hours a day, 365 days a year, and a full range of advanced care is provided, such as primary coronary intervention, pacemaker insertion, and TTM procedure. Local EMC (n=119), emergency physicians provide emergency care, and compared to regional EMC, the advanced care provided is limited or has less time to be covered. And local EMS instutusion(n=261), which may be staffed by general physicians, provides less advanced care than Local EMC, and serious diseases are often transferred to regional EMC or Local EMC [19]. Post-resuscitation guidelines recommended by international organizations (American Heart Association, European Society For Emergency Medicine) are widely accepted in Korea and are recommended for clinical use.
Study participants
This study included all EMS-treated OHCA patients with presumed cardiac etiology who were 18 years or older and who underwent TTM between January 2013 to December 2018. Patients with missing data on initial BT or survival outcomes were excluded.
Outcome measures
The primary outcome was a good neurologic status, with a Cerebral Performance Category (CPC) score of 1 (good recovery) or 2 (mild disability), and secondary outcome was survival to hospital discharge [20,21]. The CPC score and survival to discharge were classified by trained medical record reviewers employed by KCDC.
Measurements
Initial BT was defined as the measured temperature before starting TTM. Low initial BT was defined as <35.5°C, normal initial BT as ≥35.5°C and <37.5°C, and high initial BT as ≥37.5°C [6,22,23]. We collected demographic characteristics including age, sex, and past medical history (diabetes mellitus, hypertension, and heart disease), the season of arrest, location of arrest (public or other), urbanization level of residential area (metropolitan or rural), bystander witness status (no or yes), primary cardiac rhythm assessed by EMS provider (shockable or non-shockable), EMS response time interval (elapsed time from call to EMS arrival at the scene), EMS scene time interval (elapsed time from EMS arrival to departure from the scene), and EMS transport time interval (elapsed time from departure from the scene to arrival in the ED), level of ED, post-resuscitation care (percutaneous coronary intervention and extracorporeal membrane oxygenation). We also collected TTM characteristics including method of cooling (external conventional cooling, external device cooling, intravascular cooling, intracavitary cooling), target temperature (moderate hypothermia as target temperature<35.5°C and normothermia as target temperature≥35.5°C), time from ED arrival to TTM initiation, TTM initiation to the target temperature, target temperature to TTM termination, a total duration of TTM.
Statistical analysis
Demographic findings and outcomes were analyzed by initial BT. The continuous variables were compared Wilcoxon rank-sum test, and categorical variables were compared using the chi-squared test. Multivariable logistic regression analysis was conducted to estimate the effect of initial BT on survival outcomes for all study patients, and to calculate the adjusted odds ratios (aOR) and 95% confidence intervals (CI) after adjusting for age, sex, past medical history (diabetes mellitus, hypertension, and heart disease), location of arrest, witness, bystander CPR, initial rhythm, EMS response time interval, level of ED and percutaneous coronary intervention.
To estimate the effect of initial BT changed by initial cardiac rhythm, we added an interaction term of initial BT and initial ECG rhythm at cardiac arrest to the multivariable logistic regression model. A P<0.05 was considered significant for all analyses. All statistical analysis was performed using SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Demographics
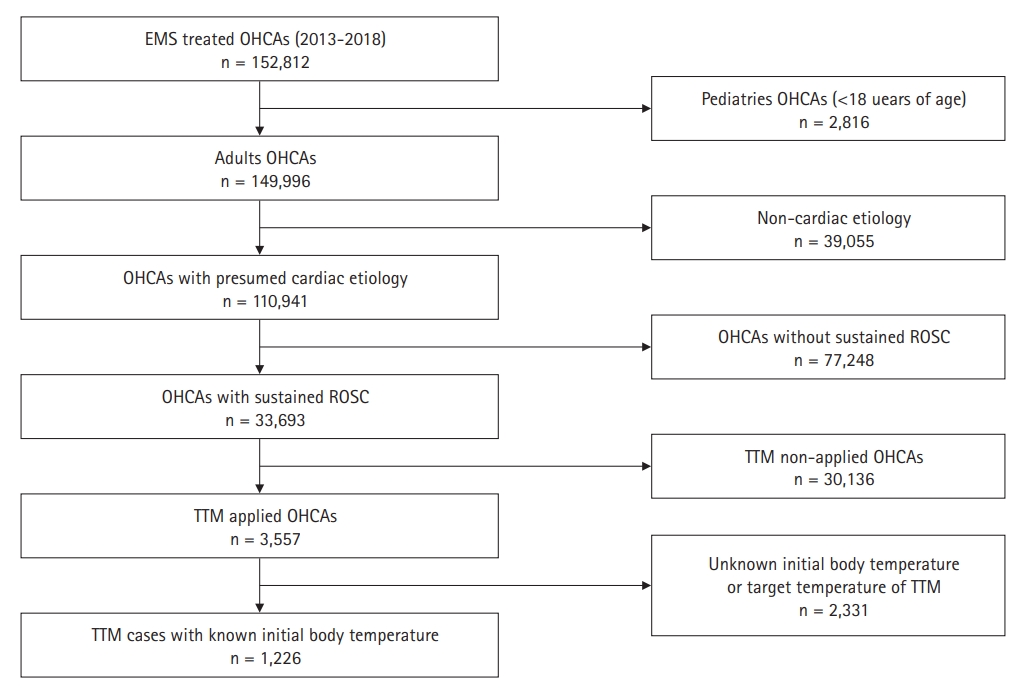
Of the 152,812 OHCA patients, 1,226 were admitted to the hospital after survival and included in the analysis (Fig. 1). We excluded patients who were younger than 18 years of age (n=2,816), whose OHCA had a non-cardiac cause (n=39,055), OHCAs without sustained return of spontaneous circulation (ROSC; n=77,248), for whom TTM was not conducted (n=30,136), or whose initial BT was unknown (n=2,331).
Demographic characteristics by initial BT at TTM are shown in Table 1. The proportion of shockable rhythm was the lowest in the low BT group (35.9% in low, 61.5% in normal, and 50.5% in high BT group, P<0.001). Median (interquartile range, IQR) time from TTM initiation to target temperature was 100 minutes (IQR, 30 to 230 minutes) in the low BT group, 195 minutes (IQT, 105 to 383 minutes) in the normal BT group, and 360 minutes (IQR, 225 to 596 minutes) in the high BT group (P<0.001). For patients who received therapeutic hypothermia (TTM target temperature was less than 35.5°C), the time from TTM initiation to termination is 2,280 minutes (IQR, 1,888 to 2,760 minutes) in low BT, 2,351 minutes (IQR, 1,987 to 2,720 minutes) in normal BT, and 2,445 minutes (IQR, 2,100 to 3,008 minutes) in high BT (P=0.019). Survival to discharge was 40.1%, 62.8%, and 58.1% in the low, normal, and high BT groups, respectively (P<0.001). Good neurologic recovery was 15.0%, 39.9%, and 34.3% in the low, normal, and high BT groups, respectively (P<0.001) (Table 1).
Main analysis
Patients with low initial BT were less likely to have good neurologic recovery (aOR for a good neurologic recovery, 0.36; 95% CI, 0.25 to 0.51) and had lower survival rates (aOR for survival to discharge, 0.53; 95% CI, 0.40 to 0.71) compared with those in the normal BT group. High initial BT was not significantly associated with good neurologic recovery (aOR for good neurologic recovery, 0.72; 95% CI, 0.43 to 1.22) or with survival to discharge (aOR for survival to discharge, 0.78; 95% CI, 0.49 to 1.23) (Table 2).
In interaction analysis, the low initial BT group was less likely to have good neurologic recovery and survival to discharge than the normal initial BT group, regardless of initial ECG rhythm. The negative effect of abnormal initial BT on good neurological recovery was significantly intensified in patients with initial non-shockable rhythm. For survival to discharge, the negative effect of high initial BT was significantly intensified in patients with initial non-shockable rhythm (Table 3).
DISCUSSION
We found that low initial BT was associated with poor neurologic outcomes in OHCA patients who underwent TTM. We also found that low initial BT was associated with poor neurologic recovery regardless of initial ECG rhythm at the scene. These results indicate that low BT at the initiation of TTM might reflect brain injury and has the potential to be a predictor of unfavorable neurologic outcome in OHCA patients. Therefore, when TTM is performed in OHCA patients with low initial BT, close monitoring and intensive management are necessary.
Previously, BT was not considered a predictor for neurologic recovery of OHCA patients [21,24−26]. However, BT can reflect brain damage in OHCA patients. Previous studies have shown an association between low BT at admission and unfavorable outcomes [13,14]. In addition, regardless of the initial ECG rhythm, which is a strong predictor of survival outcomes of OHCA, it was found that low initial BT was associated with poor neurologic recovery. This is thought to be due to brain global ischemia after cardiac arrest, and thereby damage to the hypothalamus that controls BT. In patients with brain damage, abnormalities in thermoregulation control are common [11,12].
Because outcomes of low initial BT patients who underwent TTM was poor, careful decision and conduction of TTM are important for those patients. It was reported that events of unintentional BT drop than target temperature during TTM treatment were associated with unfavorable neurological recovery [27]. We found that median time from initiation of TTM to target temperature was shorter in low BT group (100 minutes in low BT group, 195 minutes in normal BT group, and 360 minutes in high BT group; P<0.001), and the median time from target temperature to termination of TTM was prolonged in low BT group (2,160 minutes in low BT group, 2,100 minutes in normal BT group, and 2,080 minutes in high BT group; P=0.479). Because the low BT group stays more close to the target temperature during TTM, those patients have more possibility to BT drop during TTM. Therefore, intensive monitoring to avoid BT drop is necessary.
We found that both low initial BT and non-shockable rhythm were associated with poor outcomes and there was an interactive effect between initial BT and non-shockable rhythm. In interaction analysis, the negative effect of low initial BT and high initial BT was profound in patients with non-shockable rhythm. An initial non-shockable rhythm was a well-known predictor for poor outcome in OHCA patients [24−26]. Because these patients would have prolonged arrest time and severe global brain injury, the effect of abnormal BT might be greater than patients with a shockable rhythm. Studies for evaluating detailed protocol for post-resuscitation care including TTM to diminish brain injury for those patients are warranted.
There are some limitations to this study. First, because our study was a nationwide observational study, an exact method for measurement of BT was not identified because of the lack of information. Second, because initial BT could be directly affected by environmental factors of the place of arrest, patients with low initial BT could be heterogeneous according to environmental factors. We adjusted a place of arrest for multivariable analysis, but environmental factors could not be fully adjusted. Third, because this study is a retrospective observational study, there may be an uncontrolled potential bias compared to a prospective randomized controlled trial.
In conclusion, we found that low initial BT at TTM was associated with poor neurologic recovery in adult patients with OHCA of presumed cardiac etiology who underwent TTM. Low initial BT might reflect dysfunction of thermoregulation control, which is associated with global brain damage in OHCA patients. Our finding suggests that information about BT can be used to assess the survival outcomes in OHCA patients. Prospective studies incorporating BT as the prognostication tool are warranted. Because OHCA patients with low initial BT showed poor survival outcomes, careful decision and intensive management of TTM is necessary. Close monitoring of BT to avoid BT drop could affect survival outcomes of patients with low initial BT. Studies for evaluating delicate post-resuscitation care to improve outcomes of OHCA patients with low initial BT is warranted.